
Licensed professionals can receive the latest Listerine clinical information and patient resources.
Why add mouthrinse to your patients’ daily oral health routine?
Even with today’s increased focus on oral healthcare, including good brushing and flossing techniques, gum disease is still much more prevalent than might be expected. In fact, in the US alone, nearly 75% of adults suffer from some form of gum disease.1
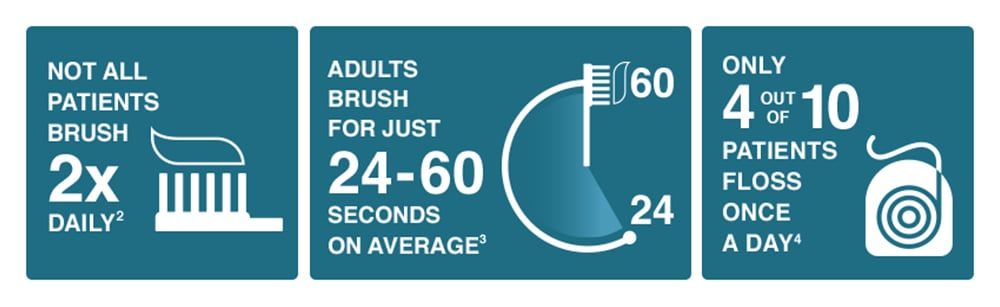
And, even though many patients do strive for good oral health, they often don’t comply fully with recommended oral care instructions. Others simply have poor habits that make plaque control difficult to achieve through brushing and flossing alone.
The good news is the majority of people are willing to do more for their oral health. A global survey of over 4000 people5* showed: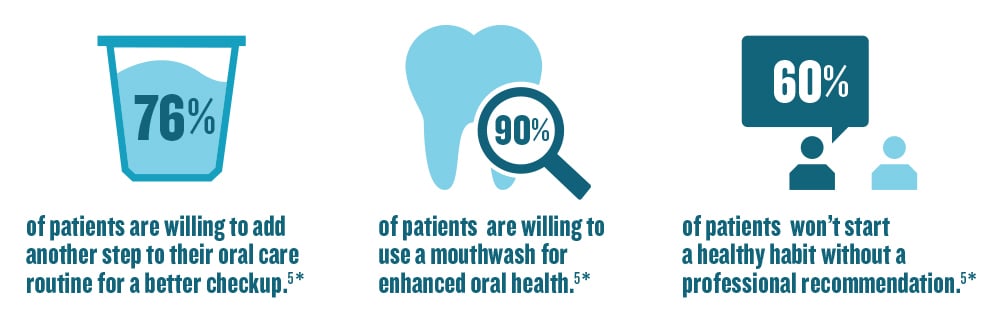
It’s clear that patients already have the desire to improve their oral health, but need more of an incentive.
Why recommend oral rinsing?
While mechanical methods (MM), like brushing and flossing, are vital to proper oral care, they may not be enough alone to control plaque.6,7 Bacteria are hiding in places where brushing, and even flossing, simply can’t reach. Appearing within minutes of brushing, bacteria double every 1-2 hours in the early stages—and within days, microbes form a complex 3-D colony that can contain hundreds of distinct species.8† Unstimulated saliva contains 5 x 107 to 1 x 108 bacteria per milliliter, and continually bathes oral surfaces with suspended microorganisms, allowing bacteria to re-colonize on teeth shortly after prophylaxis.9
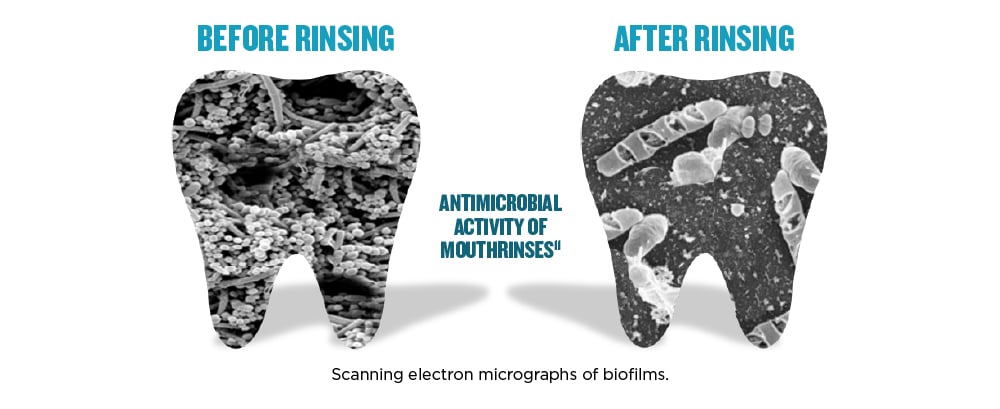
Antimicrobial mouthrinses provide benefits that brushing and flossing do not. Many are formulated with ingredients designed to reduce plaque and gingivitis—and these agents have been found to be effective against the development of plaque biofilm in multiple clinical trials.10
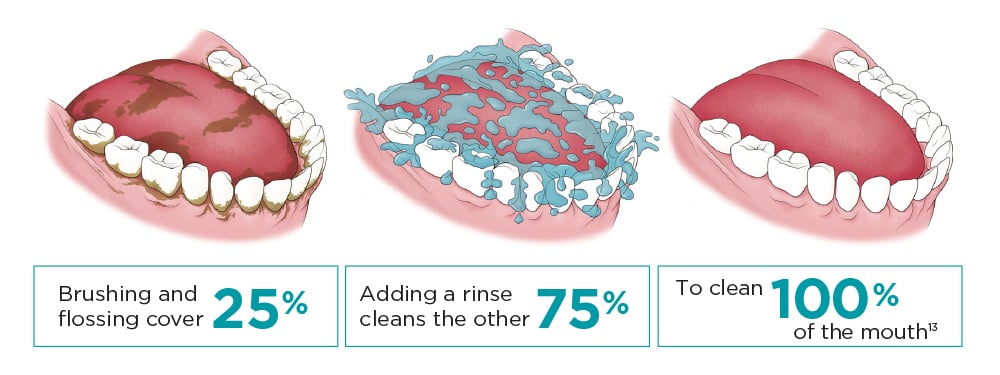
Mechanical oral hygiene techniques generally focus only on the teeth, while plaque bacteria are prevalent in the oral mucosal tissues that comprise the majority of the oral surface.12 In fact, since teeth only represent 25% of the mouth's surfaces, and mechanical methods only affect teeth, plaque biofilm is still present in the mouth even after brushing and flossing.13 For this reason, it’s important to recommend an oral health routine that attacks plaque biofilm growth from all angles, in every area of the mouth.
Fortunately, as a liquid, an antimicrobial mouthrinse used for just 30 seconds can reach all areas of the mouth and penetrate deep into plaque biofilm, killing remaining bacteria. Which means a proper oral healthcare routine that incorporates rinsing in addition to brushing and flossing can result in a virtually 100% whole-mouth clean.13
ADA recognizes the benefits of rinsing.14
In addition to the American Dental Association’s recommendations for brushing and flossing, the ADA also recognizes the benefits of rinsing twice a day with an ADA-Accepted antimicrobial mouthrinse to reduce plaque and gingivitis.14
The ADA Council on Scientific Affairs has adopted specific guidelines to earn the ADA Seal of Acceptance for the Chemotherapeutic Products for Control of Gingivitis category. The ADA set very high standards encompassing both effectiveness and safety. This included two 6-month studies showing a minimum 15% reduction in gingivitis and a mean of no less than 20% across the 2 studies, before awarding the Seal.
At the moment, only one nationally branded over-the-counter (OTC) antiseptic mouthwash has earned the ADA Seal of Acceptance to prevent plaque and gingivitis: LISTERINE® Antiseptic.15‡
Rinsing—the essential third step to better oral health.
With all this evidence, it’s clear that rinsing with an antimicrobial mouthrinse has become more than just a suggestion. It’s now become an essential third step in addition to brushing and flossing in a patient’s daily oral health routine. And, it’s a step you should be recommending to your future patients to help make their mouths healthier.
What we’ve learned:
1. What is the prevalence of gingivitis in the US?
a.) Almost 10% of the adult population
b.) Almost 25% of the adult population
c.) Almost 50% of the adult population
d.) Almost 75% of the adult population
2. What is the average brush time for adults?
a.) 24-60 seconds
b.) 35-60 seconds
c.) 45-75 seconds
d.) 60-90 seconds
3. How many patients floss at least once a day?
a.) 4 out of 10
b.) 5 out of 10
c.) 6 out of 10
d.) 7 out of 10
4. What is the benefit of using antimicrobial mouthwash in addition to mechanical methods of plaque removal?
a.) Helps prevent and reduce plaque
b.) Helps prevent and reduce gingivitis
c.) Cleans virtually 100% of the mouth
d.) All of the above
Answers: 1. d; 2. a; 3. a; 4. d.
CLINICAL STUDIES ON PLAQUE AND GINGIVITIS REDUCTION.
Explore evidence from a study about LISTERINE® Antiseptic and the reduction of plaque and gingivitis.

ADA Recognizes the Benefits of Rinsing.
Brushing and flossing are both important parts of good oral health, and the ADA recognizes the benefits of rinsing.
Why Recommend a Mouthrinse? Footnotes
*Based on self-reported data from a survey of patients in the United States, United Kingdom, Thailand, Brazil, and Japan (N=4134).
†25 species at a specific location in the biofilm, but several hundred species throughout the mouth of the same individual.
‡The ADA Council on Scientific Affairs’ Acceptance of LISTERINE® Antiseptic is based on its finding that the product is effective in helping to prevent or reduce gingivitis and plaque above the gumline, when used as directed.
References: 1. DentalPlans.com. Fast facts & figures. https://www.dentalplans.com/content/pdfs/fastfacts.pdf. Accessed August 30, 2016. 2. Bakdash B. Current patterns of oral hygiene product use and practice. Periodontal 2000. 1995;8:11-14. 3. Cancro LP, Fischman SL. The expected effect on oral hygiene of dental plaque control through mechanical removal. Periodontology 2000. 1995;8:60-74. 4. American Dental Association. Survey finds shortcomings in oral health habits. ADA Web site. Accessed August 30, 2016. 5. Study of Bold Oral Health Survey, 2015. 6. Gunsolley JC. A meta-analysis of six-month studies of antiplaque and antigingivitis agents. JADA. 2006;137:1649-1657. 7. Gunsolley JC. Clinical efficacy of antimicrobial mouthrinses. J Dent. 2010;38(I):S6-S10. 8. Marsh PD, Martin MV, Lewis MOA, Williams D. Dental Plaque. Oral Microbiology E-Book, 5th Edition. Churchill Livingstone. 2009. 80-89. 9. Liljemark WF, Bloomquist CG, Reilly BE, Lemoine JL. Growth dynamics in a natural biofilm and its impact on oral disease management. Adv Dent Res. 1997;11(1):14-23. 10. Ciancio SG. Mouthrinses and their impact on oral hygiene. Accessed March 15, 2010. 11. Data on File, Johnson & Johnson Consumer Inc. 12. Mager DL, Ximenez-Fyvie LA, Haffajee AD, Socransky SS. Distribution of selected bacterial species on intraoral surfaces. J Clin Periodontol. 2003;30(7):644-654. 13. Kerr WJS, Kelly J, Geddes DAM. The areas of various surfaces in the human mouth from nine years to adulthood. J Dent Res. 1991;70:1528-1530. 14. Learn more about mouthrinses. ADA.org Web site. Accessed September 30, 2014. 15. American Dental Association. ADA seal product report: Listerine® antiseptic. ADA Web site. https://www.ada.org/en/science-research/ada-seal-of-acceptance. Accessed May 9, 2014.
All Fields required, unless otherwise indicated
Personal Information
Step 1
Will be used as your user name
By submitting your information above, you agree that the information you provide will be governed by our site's Privacy Policy.